

Articles
- Page Path
- HOME > Urogenit Tract Infect > Volume 20(3); 2025 > Article
- Case Report Primary Bladder and Ureteral Amyloidosis Initially Diagnosed as Chronic Cystitis: A Case Report
-
Seungsoo Lee1,2
 , Dan Bee Lee1,2, Hyun Jung Lee1,3, Won Hoon Song1,2, Sung-Woo Park1,2, Jong Kil Nam1,2
, Dan Bee Lee1,2, Hyun Jung Lee1,3, Won Hoon Song1,2, Sung-Woo Park1,2, Jong Kil Nam1,2 -
Urogenital Tract Infection 2025;20(3):167-172.
DOI: https://doi.org/10.14777/uti.2550038019
Published online: December 31, 2025
1School of Medicine, Pusan National University, Yangsan, Korea
2Department of Urology, Pusan National University Yangsan Hospital, Yangsan, Korea
3Department of Pathology, Pusan National University Yangsan Hospital, Yangsan, Korea
-
Corresponding author: Jong Kil Nam Department of Urology, Pusan National University Yangsan Hospital, 20 Geumo-ro, Mulgeum-eup, Yangsan 50612, Korea Email: tuff-kil@hanmail.net
• Received: September 6, 2025 • Revised: November 14, 2025 • Accepted: November 18, 2025
Copyright © Korean Association of Urogenital Tract Infection and Inflammation
This is an open access article distributed under the terms of the Creative Commons Attribution Non-Commercial License (http://creativecommons.org/licenses/by-nc/4.0) which permits unrestricted non-commercial use, distribution, and reproduction in any medium, provided the original work is properly cited.
- 1,486 Views
- 16 Download
- 1 Crossref
Abstract
- Primary localized amyloidosis confined to the urinary tract is uncommon and frequently misinterpreted due to clinical and radiologic overlap with more prevalent conditions. We describe a 69-year-old woman who experienced recurrent gross hematuria over 2 years and underwent initial transurethral resection based on a presumptive diagnosis of chronic cystitis. Subsequent evaluation revealed a left ureteral mass with hydronephrosis, raising concern for malignancy. Histopathologic examination of both bladder and ureteral specimens demonstrated amorphous eosinophilic deposits that stained positive with Congo red and showed apple-green birefringence under polarized microscopy. Immunofluorescence confirmed λ-light-chain predominance, establishing AL (amyloid light chain)-type amyloidosis without systemic involvement. The patient underwent complete endoscopic resection and remains asymptomatic during ongoing surveillance. This case highlights the diagnostic challenges posed by localized urinary amyloidosis and underscores the importance of histologic confirmation in atypical inflammatory lesions.
HIGHLIGHTS
Primary localized urinary tract amyloidosis is rare and often mimics chronic inflammation or malignancy, leading to diagnostic delays; in this case, a ureteral mass initially presumed to be cystitis was ultimately identified as AL (amyloid light chain)-type amyloidosis through Congo red staining and λ-light-chain predominance, and complete endoscopic resection achieved symptom resolution, underscoring the importance of histologic confirmation in atypical urinary lesions.
INTRODUCTION
Primary localized amyloidosis of the urinary bladder represents an uncommon benign condition characterized by extracellular amyloid fibril deposition confined to the bladder wall. Unlike systemic forms, this entity lacks involvement of other organ systems. Clinical manifestations typically include hematuria and lower urinary tract symptoms, which can closely resemble bladder carcinoma or chronic cystitis. This similarity often leads to diagnostic uncertainty and occasionally unnecessary aggressive treatment approaches [1,2]. Given that fewer than 200 cases have been documented in the medical literature worldwide, clinicians frequently encounter difficulty distinguishing this condition from malignancy or chronic inflammatory processes during initial assessment [3].
On cystoscopic examination and imaging studies, the appearance often mimics urothelial carcinoma, with papillary or polypoid lesions that cannot be reliably differentiated based on visual characteristics alone. Chronic cystitis, by contrast, more commonly manifests as diffuse mucosal erythema or edema rather than forming discrete mass lesions [4]. Definitive diagnosis requires histopathologic evaluation using Congo red staining, which produces characteristic apple-green birefringence when viewed under polarized light [5]. Additional testing through immunohistochemistry and proteomic methods helps determine the specific amyloid subtype, with immunoglobulin light chain (AL, amyloid light chain) being the most frequently identified variant [6].
We report an unusual case involving simultaneous primary localized AL-type amyloidosis of both the bladder and distal ureter in a patient initially thought to have recurrent chronic cystitis. This presentation illustrates important diagnostic considerations that warrant attention.
CASE REPORT
A 69-year-old woman presented with intermittent gross hematuria that had persisted for approximately 2 years. She had begun experiencing intermittent gross hematuria accompanied by dysuria, frequency, and urgency around May 2023. Her medical history included a chronically atrophic right kidney, though the underlying cause remained undetermined. She had no other past medical history, including no chronic systemic diseases, autoimmune disorders, or hematologic conditions. Two years before the current presentation, she had undergone transurethral resection of bladder tumor (TUR-BT) after cystoscopy identified abnormal mucosal changes. The pathology report from that procedure described acute and chronic inflammation but found no evidence suggesting malignancy.
Her family history was unremarkable, with no known hereditary renal, hematologic, or autoimmune diseases. She denied tobacco use, alcohol consumption, or relevant occupational exposures.
Laboratory workup performed before the planned surgical intervention showed unremarkable findings. Complete blood count, serum chemistry panel, and urinalysis revealed no significant abnormalities. There were no signs of active infection or compromised renal function.
During the post–TUR-BT period, her lower urinary tract symptoms were managed medically with an α-blocker (silodosin), an anticholinergic agent (fesoterodine), and Uro-vaxom. She had been maintained on a surveillance protocol consisting of periodic cystoscopy and abdominopelvic computed tomography (CT). A follow-up CT scan performed in November 2024 identified a new mass lesion in the left distal ureter accompanied by hydronephrosis (Fig. 1). This finding prompted concern about possible malignant disease and led to the decision for surgical exploration in March 2025 (Table 1).
Written informed consent was obtained from the patient for publication of this case report and accompanying images.
The procedure was performed under general anesthesia and lithotomy position. Initial ureteroscopy was accomplished using a semirigid ureteroscope, through which a 7.5-Fr Roadrunner guidewire (Cook Medical, USA) was successfully positioned in the left ureter. Approximately 2 cm proximal to the ureteral orifice, abnormal edematous changes were noted in the mucosa (Fig. 2A and B). Flexible ureterorenoscopy (URF-V2, Olympus, Japan) was then performed to examine the upper ureter and renal pelvis, which appeared normal without additional lesions.
Because the patient’s prior transurethral resection of the bladder lesion demonstrated only chronic inflammation, and both cystoscopic and ureteroscopic evaluation in the current procedure revealed mucosal changes more suggestive of an inflammatory process rather than a malignant tumor, we elected to perform endoscopic biopsy to obtain definitive histologic confirmation rather than proceed directly with more aggressive oncologic intervention. After ureteral biopsy, a 6-Fr, 26-cm ureteral stent (Inlay Optima, USA) was placed.
Using a bipolar resectoscope (Olympus, Japan), inspection revealed yellow-to-reddish edematous mucosal alterations along the posterior bladder wall (Fig. 2C). These areas underwent transurethral resection. Following completion of the resection, a 22-Fr 3-way hematuria Foley catheter was inserted to facilitate postoperative bladder irrigation.
Microscopic examination of both the ureteral and bladder tissue specimens showed similar findings. Amorphous eosinophilic material was deposited throughout the subepithelial stroma. When Congo red stain was applied and the slides examined under polarized light, the characteristic apple-green birefringence confirmed the presence of amyloid. Immunofluorescence studies demonstrated predominant λ-light-chain restriction. Immunohistochemistry for amyloid A protein returned negative results. These findings established the diagnosis of primary localized AL (λ-type) amyloidosis (Fig. 3).
The ureteral stent was removed 2 weeks postoperatively without complications. To rule out systemic amyloidosis, comprehensive evaluation was undertaken including CT imaging of the chest, abdomen, and pelvis, along with echocardiography. Serum testing consisted of protein electrophoresis, immunoglobulin quantification, β₂-microglobulin levels, and serum free-light-chain assays. All studies showed no evidence of systemic disease involvement. The patient has remained free of symptoms, with resolution of both hematuria and dysuria. Follow-up imaging confirmed resolution of the hydronephrosis. She continues under regular surveillance with cystoscopy and imaging studies (Table 1.).
DISCUSSION
Primary localized amyloidosis affecting the bladder is an uncommon diagnosis that can closely mimic both bladder carcinoma and chronic cystitis in its presentation. In our patient, the combination of recurrent hematuria and irregular mucosal appearance initially suggested inflammatory cystitis, though the subsequent development of a ureteral mass raised concern for neoplastic disease. As described in earlier reports, cystoscopic findings showed edematous mucosa with mass-like features, while imaging demonstrated focal wall thickening and involvement of the ureter [1,3,7]. These characteristics cannot be reliably distinguished from urothelial carcinoma based on appearance alone, which makes tissue diagnosis essential.
In addition, dual involvement of both the bladder and the ureter is exceedingly rare, and only a small number of similar cases have been reported in the literature. These previous cases also emphasized that radiologic or endoscopic findings could not differentiate amyloidosis from malignancy, and histologic confirmation remained the decisive diagnostic step [1,3,7]. Our case therefore contributes additional evidence to this limited body of reports by demonstrating synchronous bladder and distal ureteral disease.
Under microscopic examination, amyloid deposits appear as acellular eosinophilic material within the submucosa and around vessel walls. The diagnosis is confirmed when Congo red staining produces apple-green birefringence under polarized microscopy [5]. Chronic cystitis, in comparison, shows widespread mucosal inflammation without forming discrete masses or demonstrating amyloid deposition [4]. Further classification through immunohistochemical or proteomic analysis helps distinguish localized disease from systemic amyloidosis. Our patient's λ-light-chain predominance confirmed localized AL-type disease, which aligns with findings from previous case series [6,8].
The underlying mechanism of localized urinary amyloidosis has not been fully elucidated, though current understanding suggests chronic mucosal irritation may trigger localized plasma-cell activation. These plasma cells produce light chains that aggregate into β-pleated amyloid fibrils [9]. This proposed mechanism could explain why many patients have a preceding history of recurrent cystitis or local inflammatory conditions. An important distinction from systemic amyloidosis, which carries a guarded prognosis, is that localized forms typically follow an indolent course and remain confined to the affected organ [10].
Treatment primarily involves complete local resection of visible deposits. Transurethral resection or laser ablation effectively removes the abnormal tissue and relieves symptoms [7]. Once the diagnosis of amyloidosis is histologically confirmed, aggressive surgical approaches such as partial or total cystectomy are not indicated. However, recurrence has been documented in approximately one-third of patients, which necessitates long-term surveillance with regular cystoscopy [2,7]. Based on these recurrence rates, most authors recommend cystoscopic follow-up every 6–12 months during the initial several years after treatment, which aligns with the surveillance strategy implemented in our patient.
Our patient's postoperative course has been favorable, with no evidence of recurrence or systemic involvement during the follow-up period. The dual-site involvement and the successful exclusion of systemic amyloidosis strengthen the clinical relevance of this report. However, the limitations of this case include the inherent constraints of a single-patient description and a relatively short duration of follow-up. This case illustrates 2 important diagnostic challenges. First, amyloidosis can occur alongside chronic inflammatory changes, which may lead to misdiagnosis as simple cystitis if Congo red staining is omitted from the pathologic evaluation. Second, ureteral involvement, as demonstrated in this patient, is particularly rare and can be mistaken for upper-tract urothelial carcinoma. Recognition of these potential pitfalls and routine application of Congo red or immunostaining techniques when evaluating atypical inflammatory lesions are crucial for accurate diagnosis.
Primary localized bladder and ureteral amyloidosis warrant consideration in patients presenting with recurrent hematuria or cystitis-like lesions that fail to respond to conservative management. Accurate diagnosis depends on histologic confirmation and determination of the amyloid subtype. Once systemic disease has been excluded, conservative endoscopic resection combined with regular surveillance offers excellent long-term outcomes.
-
Funding/Support
This study received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.
-
Conflict of Interest
The authors have nothing to disclose.
-
Author Contribution
Conceptualization: SL, JKN; Data curation: SL, DBL, HJL; Formal analysis: SL, DBL, WHS; Methodology: SL, WHS, SWP; Project administration: SWP, JKN; Visualization: SL, HJL; Writing - original draft: SL, DBL, HJL; Writing - review & editing: SWP, JKN.
NOTES
Fig. 1.
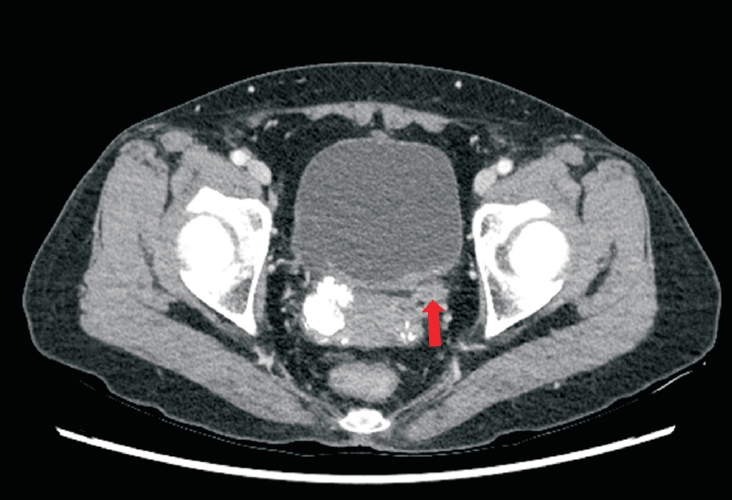
Contrast-enhanced computed tomography showing focal wall thickening of the left lower ureter (red arrow).
Fig. 2.
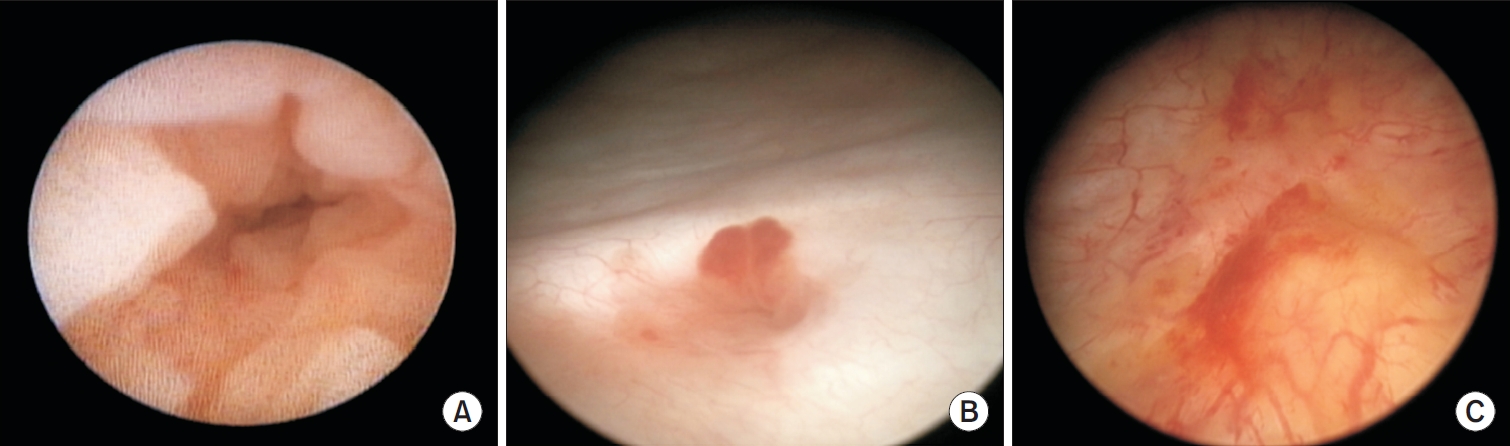
(A) Ureteroscopic view showing edematous mucosal changes in the lower ureter. (B) Endoscopic view showing an abnormal mucosal lesion at the left ureterovesical junction. (C) Yellow-to-reddish edematous mucosal lesions on the posterior wall of the bladder.
Fig. 3.
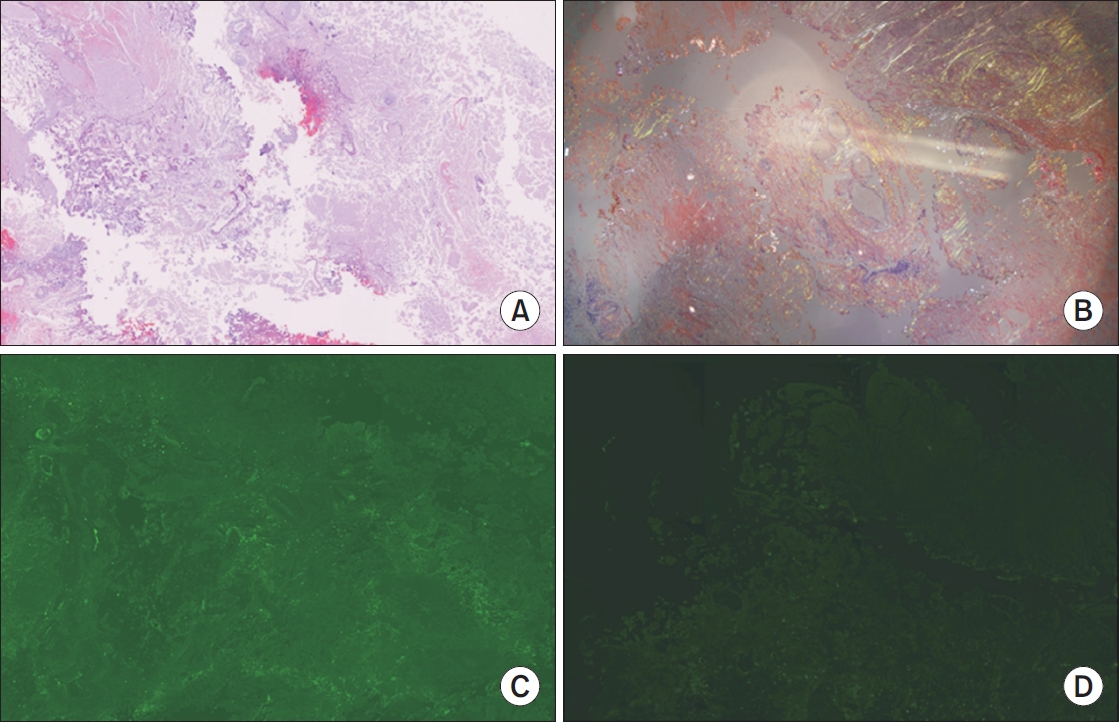
(A) Photomicroscopy image (hematoxylin and eosin stain, ×40) of amyloidosis. (B) Congo red staining demonstrating amyloid deposits with apple-green birefringence under polarized light (×40). (C) Immunohistochemical staining demonstrating λ lightchain positivity within the amyloid deposits (×40). (D) Immunohistochemical staining demonstrating negative κ light chain expression within the amyloid deposits (×40).
Table 1.
Timeline of key clinical events
- 1. Tirzaman O, Wahner-Roedler DL, Malek RS, Sebo TJ, Li CY, Kyle RA. Primary localized amyloidosis of the urinary bladder: a case series of 31 patients. Mayo Clin Proc 2000;75:1264-8.ArticlePubMed
- 2. Riefolo M, Conti M, Longhi S, Fabbrizio B, Leone O. Amyloidosis: what does pathology offer? The evolving field of tissue biopsy. Front Cardiovasc Med 2022;9:1081098.ArticlePubMedPMC
- 3. Ng CY, Huang WH, Huang HC, Wang LJ, Lee SY. Localized bladder amyloidosis mimicking bladder carcinoma. Kidney Int 2014;85:1245.ArticlePubMed
- 4. Busuttil A, Moghimi A. Localised primary amyloidosis of the bladder mimicking carcinoma. Pathology 2020;52:58-62.Article
- 5. El-Meanawy A, Mueller C, Iczkowski KA. Improving sensitivity of amyloid detection by Congo red stain by using polarizing microscope and avoiding pitfalls. Diagn Pathol 2019;14:57.ArticlePubMedPMCPDF
- 6. Giannini G, Nast CC. An organ system-based approach to differential diagnosis of amyloid type in surgical pathology. Arch Pathol Lab Med 2020;144:379-87.ArticlePubMedPDF
- 7. Yanada BA, Soputro NA, Dias BH. Primary localised bladder amyloidosis - a case report with review of the literature. Urol Case Rep 2022;43:102072.ArticlePubMedPMC
- 8. Abildgaard N, Rojek AM, Møller HE, Palstrøm NB, Nyvold CG, Rasmussen LM, et al. Immunoelectron microscopy and mass spectrometry for classification of amyloid deposits. Amyloid 2020;27:59-66.ArticlePubMed
- 9. Picken MM. The pathology of amyloidosis in classification: a review. Acta Haematol 2020;143:322-34.ArticlePubMedPDF
- 10. Merlini G, Dispenzieri A, Sanchorawala V; Schönland SO, Palladini G, Hawkins PN, et al. Systemic immunoglobulin light chain amyloidosis. Nat Rev Dis Primers 2018;4:38.ArticlePubMedPDF
REFERENCES
Figure & Data
REFERENCES
Citations
Citations to this article as recorded by 
- Primary Localized Amyloidosis of the Urinary Bladder Mimicking Urothelial Carcinoma: A Case Report
Gassan M Salih, Saad Masood, Filip Kondylis
Cureus.2026;[Epub] CrossRef
 ePub Link
ePub Link Cite
CitePrimary Bladder and Ureteral Amyloidosis Initially Diagnosed as Chronic Cystitis: A Case Report
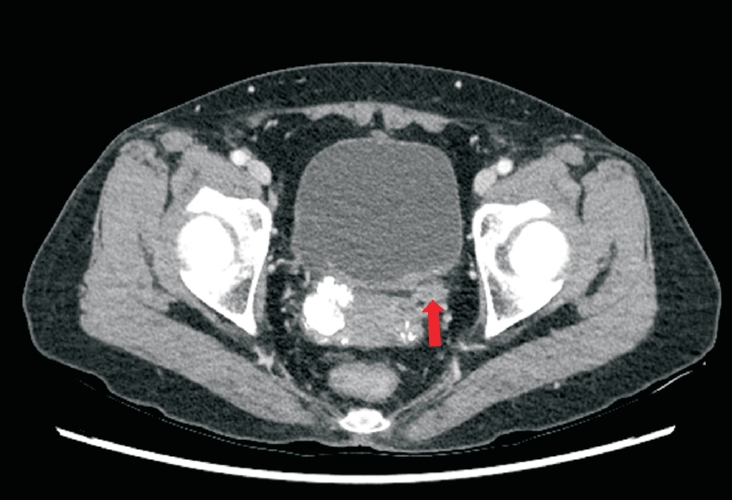

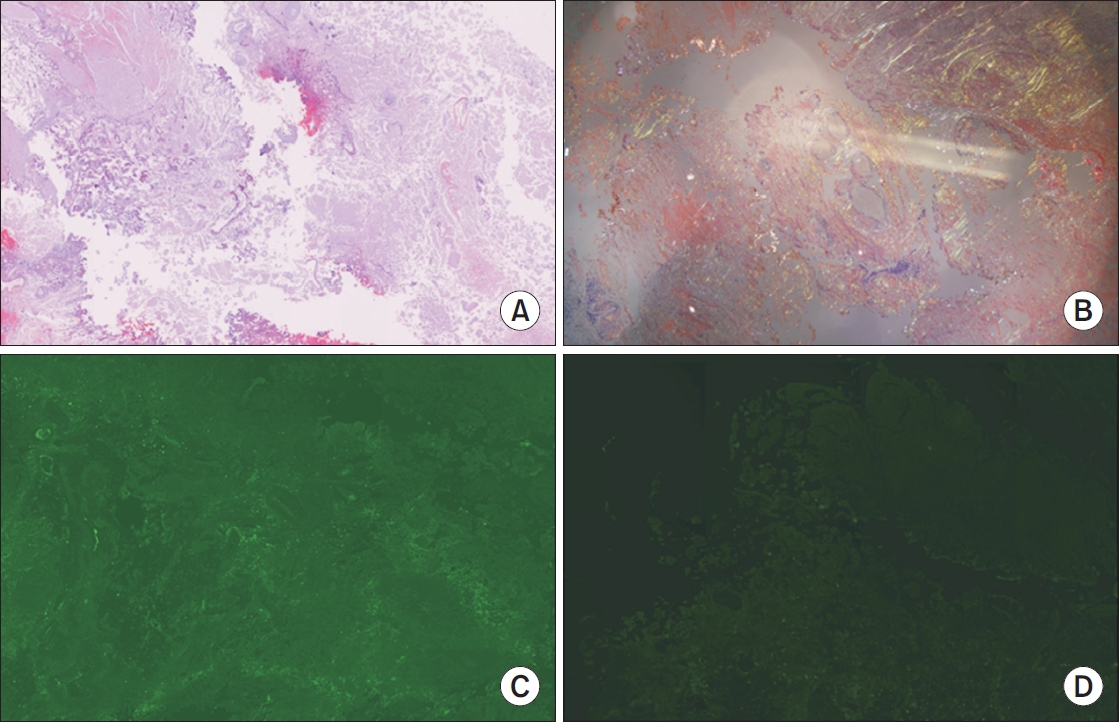
Fig. 1. Contrast-enhanced computed tomography showing focal wall thickening of the left lower ureter (red arrow).
Fig. 2. (A) Ureteroscopic view showing edematous mucosal changes in the lower ureter. (B) Endoscopic view showing an abnormal mucosal lesion at the left ureterovesical junction. (C) Yellow-to-reddish edematous mucosal lesions on the posterior wall of the bladder.
Fig. 3. (A) Photomicroscopy image (hematoxylin and eosin stain, ×40) of amyloidosis. (B) Congo red staining demonstrating amyloid deposits with apple-green birefringence under polarized light (×40). (C) Immunohistochemical staining demonstrating λ lightchain positivity within the amyloid deposits (×40). (D) Immunohistochemical staining demonstrating negative κ light chain expression within the amyloid deposits (×40).
Fig. 1.
Fig. 2.
Fig. 3.
Primary Bladder and Ureteral Amyloidosis Initially Diagnosed as Chronic Cystitis: A Case Report
| Date/period | Event |
|---|---|
| May 2023 | Onset of intermittent gross hematuria accompanied by dysuria, frequency, and urgency |
| August 2023 | TUR-BT performed; pathology showed acute and chronic inflammation without malignancy |
| September 2023 – October 2024 | Surveillance with periodic cystoscopy and abdominopelvic CT |
| Persistent urinary symptoms managed with medication | |
| November 2024 | Follow-up CT revealed left distal ureteral wall thickening with hydronephrosis, raising suspicion of malignancy |
| March 2025 | Ureteral biopsy with transurethral resection of bladder performed |
| March–April 2025 | Systemic amyloidosis evaluation (CT chest/abdomen/pelvis, echocardiography, SPEP/IFE, β2- microglobulin, serum free light chains) → No evidence of systemic involvement |
| Current status | Hematuria, hydronephrosis resolved; under scheduled cystoscopic and imaging surveillance |
Table 1. Timeline of key clinical events
TUR-BT, transurethral resection of bladder tumor; CT, computed tomography; SPEP/IFE, serum protein electrophoresis/immunofixation electrophoresis.

