
Articles
- Page Path
- HOME > Urogenit Tract Infect > Volume 18(3); 2023 > Article
- Original Article Impact of Microbial Infection on Sperm Parameters of Seminal Bacteria in Asymptomatic Subfertile Males
-
Sae Byuk Chang1
 , Tae Jin Kim2, Tae Heon Kim1, Seung-Ryeol Lee1, Young Kwon Hong1, Dong Soo Park1, Sun-Mi Cho3, Dong Hyeon Lee4, Young Dong Yu1,5,
, Tae Jin Kim2, Tae Heon Kim1, Seung-Ryeol Lee1, Young Kwon Hong1, Dong Soo Park1, Sun-Mi Cho3, Dong Hyeon Lee4, Young Dong Yu1,5, -
Urogenital Tract Infection 2023;18(3):82-92.
DOI: https://doi.org/10.14777/uti.2023.18.3.82
Published online: December 31, 2023
1Department of Urology, Bundang CHA Hospital, CHA Medical University College of Medicine, Seongnam, Korea
2Department of Urology, Il-san CHA Hospital, CHA Medical University College of Medicine, Goyang, Korea
3Department of Laboratory Medicine, Bundang CHA Hospital, CHA Medical University College of Medicine, Seongnam, Korea
4Department of Physiology, CHA Medical University College of Medicine, Seongnam, Korea
5Department of Male Infertility and Urology, Fertility Center of Bundang CHA Hospital, Seongnam, Korea
-
Correspondence to: Young Dong Yu, , Department of Urology, Bundang CHA Hospital, CHA Medical University College of Medicine, 59 Yatap-ro, Bundang-gu, Seongnam 13496, Korea, Tel: +82-31-780-5350, Fax: +82-31-780-4959, E-mail: danielyu0714@gmail.com
• Received: August 18, 2023 • Revised: October 14, 2023 • Accepted: October 15, 2023
Copyright © 2023, Korean Association of Urogenital Tract Infection and Inflammation. All rights reserved.
This is an open-access article distributed under the terms of the Creative Commons Attribution Non-Commercial License (http://creativecommons.org/licenses/by-nc/4.0) which permits unrestricted non-commercial use, distribution, and reproduction in any medium, provided the original work is properly cited.
- 1,294 Views
- 14 Download
Abstract
-
Purpose This study examined the effects of asymptomatic bacteriospermia on the semen quality of subfertile males. The types of bacteria and their antibiotic susceptibility were also analyzed.
-
Materials and Methods Semen was collected and analyzed from 510 subfertile males. One hundred and seventy-nine males showed bacteriospermia, while 331 males did not. The bacterial species, sperm parameters, hormone levels, underlying disease, and lifestyle patterns were compared between the two study groups.
-
Results The bacteriospermic males showed significantly higher rates of leukocytospermia (p=0.001) and deoxyribonucleic acid (DNA) fragmentation than the non-bacteriospermic males. Sperm motility was significantly lower in the bacteriospermic males than in non-bacteriospermic males. The most common
-
Conclusions Bacteriospermia decreased the sperm concentration, motility, normal morphology, and vitality. P. bivia is the most commonly observed bacteria in subfertile males. Appropriate antibiotic therapy of seminal bacteria species had a strong positive impact on improving the semen parameters.
INTRODUCTION
Male subfertility could result from multiple factors and represents the status of reduced fertility for a prolonged period (more than 12 months) of undesired non-conception. In contrast, the term is often used synonymously with infertility [1]. Male infertility affects 1 in 20 men and contributes to approximately half of all infertile cases [2]. The most commonly observed form of male subfertility is oligoasthenoteratozoospermia, which implies improper seminal profiles accompanying decreased sperm count and motility with increased abnormal morphology of sperma-tozoa [1]. Genitourinary tract infections (GUI) negatively influence the seminal quality, and approximately 6-44% of male infertility cases are related to GUI and bacteriospermia. In contrast, bacteriospermia is defined as the bacterial presence of ≥1,000 colony-forming units (CFU)/ml in human ejaculate [3]. Although some studies failed to prove a significant association between bacteriospermia and seminal inflammation [4,5], acute or chronic GUI might result in an inflammatory condition accompanying leukocyto-spermia, the abnormally high presence of leukocytes, which is generally defined as >1×106 leukocytes in seminal fluid [6]. GUI may cause reduced spermatozoa function and the entire spermatogenesis process because of the direct spermatotoxic effect of bacteria, elevated oxidative stress with reactive oxygen species, and deoxyribonucleic acid (DNA) fragmentation of spermatozoa [6]. Lipopolysaccharide (LPS) is a major component of the Gram-negative bacterial cell wall. LPS reduces the intracellular cyclic-adeno-sine-monophosphate, leading to elevated reactive oxygen species (ROS) production and sperm membrane disruption [7]. DNA fragmentation induced by seminal bacterial infection may cause congenital defects and fetal spontaneous abortion, and previous studies presented some bacterial species, including Chlamydia trachomatis (C. trachomatis), Ureaplasma urealyticum (U. urealyticum) and Mycoplasma species, are associated with the DNA fragmentation of spermatozoa [8]. Bacterial infections can also result in sperm-bacterial interactions, leading to sperm agglu-tination. This sperm-bacterial agglutination causes the production of a biofilm that can accommodate more vulnerable surroundings for further bacterial colonization [9]. The impact of seminal bacteria on semen quality has not been fully exposed, and it is unclear if seminal bacterial infection in asymptomatic males is associated with male subfertility [10]. Moreover, the bacterial species-specific impacts on sperm parameters and related antibiotic treatment needs in asymptomatic males are controversial [11]. Thus, this study examined the effects of bacteriospermia on semen quality in subfertile males by analyzing the sperm parameters before and after antibiotic treatment. This study also evaluated the types of seminal bacteria and their antibiotic susceptibility.
MATERIALS AND METHODS
The study was a single-center retrospectively designed study of 510 subfertile males attending the Fertility Center of Bungang CHA Hospital from January 2022 to December 2022. A subfertile male was defined as a male who had unwanted non-conception for more than one year while continuing unprotected regular sexual intercourse with his female spouse. All study participants showed at least one impaired sperm parameter according to the initial semen test with reference to the World Health Organization 2010 criteria. The patients with symptomatic GUI, azoospermia, genetic disorders, anatomical abnormalities, and auto-immune disease-related subfertility were excluded. The sociobehavioural and clinical parameters of the study participants, including age, underlying diseases, previous history of genital surgery, previous hormone treatment history, smoking and alcohol consumption history, currently taking prescribed medications, and microscopic hematuria grade, were reviewed. Personal medical data collection and all clinical procedures were conducted according to recent relevant guidelines. The Ethics Committee of the CHA Medical University approved this study (registration number 2023-06-021). Signed informed consent was obtained from all study participants regarding the use of individual medical information.
All study participants underwent semen analysis and multiplex polymerase chain reaction (PCR) tests for bacteriospermia twice: on the first visit to the clinic and three months after the initial visit. At their first visit, all subfertile males included in this study were instructed to sustain their water intake at 2-3 liters/day to minimize the possible GUI risk. Semen sample collections were undertaken at the clinic using sterile, non-toxic containers after three to five days of sexual abstinence. All study subjects urinated and washed their hands and external genitalia with disinfectant tissues twice to avoid unintended contamination during semen collection. All semen samples were analyzed 30 minutes after collection to maintain semen liquefaction. The analyzed semen parameters include the semen volume, sperm concentration, motility (total and progressive motility), morphology, vitality, and DNA fragmentation of spermatozoid. For DNA fragmentation analysis, the sperm chromatin dispersion was reviewed. The spermatozoa were classified as spermatozoa with fragmented DNA if they showed small halos or without halos or spermatozoa with cell degradation. Leukocytospermia was determined to be more than 1×106 leukocytes per ml of semen.
The current study defined bacteriospermia as ≥1,000 CFU per ml of semen. The bacterial species were evaluated by extracting the microbial DNA using QIAamp DNA Blood Mini Kit (Qiagen) according to the manufacturer’s instructions. After microbial DNA extraction, bacterial strain specific multiplex real-time PCR (qPCR) was performed using NextGene™ STI Detection Kit (Ewon Reference Laboratory) to detect the following bacterial species: Neisseria gonorr-hoeae, C. trachomatis, Ureaplasma parvum (U. parvum), U. urealyticum, Mycoplasma genitalium (M. genitalium), Mycoplasma hominis (M. hominis), Tricho-monas vaginalis (T. vaginalis), Treponema pallidum (T. pallidum), Herpes simplex type-1 (HSV1), Herpes simplex type-2 (HSV2), Gardnerella vaginalis (G. vaginalis), Candida albicans (C. albicans), Escherichia coli (E. coli), Haemophilus ducreyi (H. ducreyi), Atopobium vaginae (A. vaginae), Streptococcus agalactiae (S. agalactiae), Pseudomonas aeruginosa (P. aeruginosa), Klebsiella pneumoniae (K. pneumoniae), Enterococcus faecalis (E. faecalis), Staphylococcus aureus (S. aureus), Bacteroides fragilis (B. fragilis), Mobiluncus curtisii (M. curtisii), Mobiluncus mulieris (M. mulieris), and Prevotella bivia (P. bivia). The identified bacterial species were tested for their antibiotic susceptibility. The antibiotic susceptibility of Ureaplasma and Mycoplasma species was evaluated using a conventional available liquid culture medium-based Mycoplasma IST-2 Kit (BioMerieux) accor-ding to the manufacturer’s sensitivity interpretation guide-lines. For the other bacterial species, minimal inhibitory concentration (MIC) was measured to determine the antibiotic susceptibility using the Clinical Laboratory Standards Institute disc diffusion method by measuring the annular radius of the inhibition zones for antimicrobial agents used. In contrast, the test results were interpreted and classified as sensitive, intermediate, and resistant. After the antibiotic susceptibility evaluation, each bacterio-spermic male was treated with at least one commercially available antibiotic confirmed to be sensitive in preliminary susceptibility testing for the specific pathogen, even though the bacteriospermic males were asymptomatic regarding GUI.
A Shapiro–Wilk normality test was performed to evaluate the normal distribution of the clinical variables. A student’s t-test was used to compare the normally distributed variables, and a Mann–Whitney U-test was conducted for the variables with abnormal distribution. Univariate and multivariate logistic regression analyses with odds ratios were performed to evaluate the significant bacterial species for each semen parameter; p-values ≤0.05 were considered significant. All statistical data analyses were performed with SPSS version 24.0 (SPSS Inc.).
RESULTS
This study included 510 subfertile male patients. Table 1 lists the baseline socioclinical characteristics of the study subjects. Among these subfertile males, 331 males showed sterile semen according to qPCR tests, and the other 179 males were positive with at least one bacterial species, whereas 21 of them had ≥2 microbial presences (multi-mic-ro-bial) in semen. All study subjects underwent qPCR tests for urinary pathogens to exclude a potential hindrance from bacteriuria to seminal microbial features. No pathologic bacterial presence was confirmed in all collected urine samples. Moreover, no patient accompanied lower urinary tract symptoms at the time of evaluation. The mean age of the subfertile males was 36.6 years, and the incidence of previous genital surgery history, including varicocelec-tomy, spermatocelectomy, and orchiopexy, was similar in the two study groups (p=0.797). Both study groups showed similar results regarding initial hormone levels, including follicular stimulating hormone (FSH), luteinizing hormone (LH), total testosterone, and prolactin. Microscopic hema-turia was observed more commonly in bacteriospermic males (64.2%) compared to non-bacteriospermic males (3.0%) (p<0.001). Bacteriospermic patients had a significantly larger number of patients (76.5%) with excessive alcohol use (>15 drinks/week) than non-bacteriospermic patients (30.5%) (p<0.001), but no significant differences in smoking history were observed between the two groups (p=0.576). Non-bac-teriospermic patients had a significantly larger number of patients (24.2%) under 5-alpha reductase inhibitor (5ARI) treatment to manage androgenic alopecia compared with 16.2% of bacteriospermic patients (p=0.039).
Among the 179 bacteriospermic subfertile males, 88.3% of patients had a mono-microbial infection. In contrast, the other 11.7% of patients had a multi-microbial infection (Table 1, Fig. 1). The most frequently observed seminal pathogens were P. bivia (41.3%), U. urealyticum (13.4%), and U. parvum (13.4%). Other commonly identified bacterial species were E. faecalis (9.5%), S. agalactiae (8.9%), and M. genitalium (6.1%). M. curtisii, A. vaginae, and C. trachomatis showed seminal infection rates of 2.2%.
Table 2 lists the antibiotic susceptibility profiles of seminal pathogens confirmed from the subfertile males. All of the cases with P. bivia infection showed 100% sensitivity to metronidazole, ertapenem, piperacillin/tazobactam, and clindamycin, but ampicillin showed the highest resistance rate (31.1%) among the tested antibiotics. Among the microorganisms of the family Mycoplasmataceae, Urea-plasma species were completely susceptible to amikacin and doxycycline. On the other hand, one case of an M. genitalium infection (9.1%) was resistant to doxycycline. S. agalactiae were 100% sensitive to ampicillin, amoxicillin, ceftriaxone, ertapenem, and piperacillin/tazobactam, but E. faecalis were 100% resistant to ceftriaxone. All C. trachomatis cases showed the highest sensitivity (100%) with clarithromycin, amikacin, and doxycycline.
Table 3 lists the pre- and post-antibiotic treatment results for each bacterial species. All seminal bacterial infection cases were resolved after the initial antimicrobial treatment, but U. parvum presented the highest reinfection rate (31.8%) three months after the antimicrobial treatment. Regarding Ureaplasma species and M. genitalium cases, the total motility, progressive motility, leukocytospermia, and DNA fragmentation were improved significantly three months after the initial antibiotics treatment. After the initial antibiotics treatment of P. bivia, all sperm parameters were significantly improved except normal morphology, and no reinfection cases were observed during the three-month follow-up period. Leukocytospermia was improved significantly in all bacteriospermia cases after the initial antimicrobial treatment. The sperm vitality was improved after the antibiotic treatment in P. bivia and E. faecalis infection cases. The antimicrobial treatment increased the normal morphology of sperm only in the G. vaginalis and S. agalactiae infection cases. The eradication of seminal infection did not result in significant variations of the semen volume in all bacteriospermic cases.
Logistic regression analyses were undertaken to evaluate the predictors for specific semen parameters, and Table 4 lists the results. Regarding the decreased sperm concen-tration and vitality, P. bivia and E. faecalis were identified as independent predictors. There was no significant predictor identified in terms of a normal morphology. The seminal infection of U. parvum, U. urealyticum, M. genitalium, and P. bivia were associated with impaired sperm motility. S. agalactiae was associated with impaired normal morphology in univariate analysis, but it has lost independent predictor status in multivariate analysis. U. parvum, U. urealyticum, and P. bivia were associated with pathologically high DNA fragmentation of spermatozoa.
DISCUSSION
Male GUI and its adverse effect on sperm parameters have been discussed in many papers but remain controversial [12]. This study examined subfertile males with bacteriospermia and evaluated the prevalence of bacteriospermia among subfertile males and the negative effect of microbial infection of the male genital tract on the sperm parameters by analyzing the semen quality before and after antibiotics treatment. The results showed that 35.1% of subfertile males had a seminal bacterial infection, and adequate antibiotic treatments of specific seminal bacteria improved some sperm parameters. The current study showed bacterio-spermic males had significantly more impaired sperm quality than non-bacteriospermia males in total and progressive sperm motility, DNA fragmentation, and normal morpho-logy. Although no specific bacterial species were associated with impaired semen volume according to logistic regression analyses, the mean semen volume was increased in overall bacteriospermic males after antibiotics treatment regardless of infected bacterial types. This could be due to the increased daily water intake in study subjects [13] because all subfertile males included in the study were educated to maintain a water intake of 2-3 liters/day because drinking an adequate amount of water may prevent GUI [14].
Previous studies suggested the mechanism of impaired sperm quality induced by GUI with various bacterial species. In this study, the most commonly observed microorganism in bacteriospermic males was P. bivia, an anaerobic gram-negative microorganism suggested to be related to bacterial vaginosis and GUI. This result differed from previous studies, including Eini et al. [15] and Domes et al. [16], who reported that E. faecalis was the most detected bacterial species in the semen of subfertile males. The differences in dominant seminal bacterial species must be derived from the variations of microbial distribution in the vaginal flora of the study subjects’ female spouses. P. bivia frequently incorporates and stimulates the development of multi-microbial biofilms produced initially by GV that subsequently promote antibiotic resistance [17]. On the other hand, all P. bivia infection cases in this study showed metronidazole sensitivity, indicating no antibiotic-resistant biofilm formation might be accompanied. Moreover, a recent meta-analysis by Farahani et al. [18] reported the negative effect of Prevotella on sperm quality. The result was similar to the outcomes of the present study. The study results showed that all sperm parameters except normal morphology were improved significantly after the initial antibiotics treatment for P. bivia infection. Moreover, P. bivia was an independent predictor of sperm concentration, motility, vitality, and DNA fragmentation. Thus, a P. bivia infection in bacteriospermic subfertile males should be evaluated thoroughly, and eradicating P. bivia by proper antibiotic treatment, such as metronidazole, is recom-mended. Nevertheless, the significance of P. bivia as the dominant seminal microbial species in bacteriospermic subfertile males should be evaluated further with concurrent analysis of the vaginal flora of female spouses in a future study.
The current study investigated two Mycoplasma and Ureaplasma species, which are M. genitalium, M. hominis, U. parvum, and U. urealyticum, respectively. On the other hand, the influence on the sperm parameters by each Ureaplasma serovar was not analyzed separately. The negative role of Ureaplasma and Mycoplasma species on male infertility has been reported. Bai et al. [19] suggested infertile males carrying genitourinary infection by pathogenic bacterial species, including C. trachomatis, Ureaplasma, and Mycoplasma species, had a lower sperm concentration and higher semen leukocyte counts than pathogen-negative males. In this study, appropriate antibiotic treatment of U. parvum, U. urealyticum, and M. genitalium increased sperm motility and DNA fragmentation in subfertile males. Hence, the eradication of these bacterial species is recommended.
Non-bacteriospermic subfertile males of this study had significantly greater rates of 5ARI intake for androgenic alopecia treatment, which is similar to a previous study [20] that reported that dutasteride decreases the risk of urinary tract infection in benign prostate hyperplasia patients during the four-year follow-up. Although the association between 5ARI use and reduced bacteriospermic risk was observed, the 5ARI treatment should be applied carefully in subfertile males because even low-dose-5ARI treatment for male pattern alopecia might impair the semen quality [21].
The bacteriospermic males of this study had higher rates of heavy alcohol consumption, whereas alcohol consump-tion caused abnormal morphological changes in sperm [22]. Therefore, all study subjects are recommended to quit or minimize (less than five drinks/week) alcohol consumption during the follow-up period.
This study had some limitations. Additional evaluations, including the semen ROS level, long-term semen quality variations, and vaginal flora of female spouses, were not performed because of the single-center retrospective nature with a relatively small number of samples. Thus, further studies with a larger sample size, long-term follow-up, and correlations with the female vaginal flora will be needed to confirm the current findings. Despite these limitations, this study showed that appropriate antibiotic therapy for asymptomatic bacteriospermia promotes significant impro-vements in the semen quality of subfertile males.
CONCLUSIONS
This study suggests that asymptomatic bacteriospermia in subfertile men has detrimental effects on sperm quality. Moreover, proper antibiotic therapy of those bacteria species, particularly P. bivia, improved the semen para-meters. To the best of the authors’ knowledge, this study is the first to present the clinical importance of P. bivia infections in male fertility. Therefore, routine analysis of bacteriospermia and subsequent antibiotic treatments should be performed in subfertile males.
-
CONFLICT OF INTEREST
No potential conflict of interest relevant to this article was reported.
-
FUNDING
No funding to declare.
-
AUTHOR CONTRIBUTIONS
S.B.C. designed the study, analyzed and interpreted the clinical data, and wrote and revised the manuscript. T.J.K., T.H.K., S.R.L., D.S.P., and S.M.C. collected the clinical data and engaged in patient follow‑up. D.H.L. analyzed and interpreted the clinical data. Y.D.Y. designed and supervised the project and revised the manuscript. All the listed authors have participated actively in the study. All authors read and approved the final manuscript.
NOTES
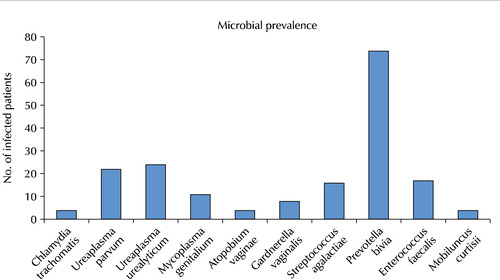
Table 1
Basic characteristics of the subfertile males (n=510)
Values are presented as mean±standard deviation (range), number (%), or mean±standard deviation.
LUTS: lower urinary tract symptoms, FSH: follicle-stimulating hormone, LH: luteinizing hormone, DNA: deoxyribonucleic acid, RBCs/HPF: red blood cells/high-power field, PCR: polymerase chain reaction, HSV1: Herpes simplex type-1, HSV2: Herpes simplex type-2, –: not available.
a)p-vlaues <0.05 are printed in bold characters. b)Multi-microbial indicates equal or more than 2 bacterial species present in body fluid. c)1 drink is equivalent to 1 glass of wine or 1 single spirit. d)5-alpha reductase inhibitor was used for the treatment of androgenic alopecia.
Table 2
Antibiotic sensitivity of pathogens detected in urine or semen samples of subfertile males
Values are presented as number (%).
C. trachomatis: Chlamydia trachomatis, U. parvum: Ureaplasma parvum, U. urealyticum: Ureaplasma urealyticum, M. genitalium: Mycoplasma genitalium, G. vaginalis: Gardnerella vaginalis, A. vaginae: Atopobium vaginae, GBS: Streptococcus agalactiae, P. bivia: Prevotella bivia, E. faecalis: Enterococcus faecalis, M. curtisii: Mobiluncus curtisii, N/A: not applicable, –: not available.
Table 3
Pre- and post-antibiotics treatment semen parameters in subfertile males with bacteriospermiaa)
Values are presented as mean±standard deviation or number (%).
U. parvum: Ureaplasma parvum, U. urealyticum: Ureaplasma urealyticum, M. genitalium: Mycoplasma genitalium, G. vaginalis: Gardnerella vaginalis, Tx: treatment, DNA: deoxyribonucleic acid, A. vaginae: Atopobium vaginae, GBS: Streptococcus agalactiae, P. bivia: Prevotella bivia, E. faecalis: Enterococcus faecalis, M. curtisii: Mobiluncus curtisii, C. trachomatis: Chlamydia trachomatis, –: not available.
a)Genitourianry tract bacterial presence indicates bacterial infection confirmed in urine or semen samples. b)Semen parameters are presented in mean±standard deviations. c)Recurrence rate was evaluated at 3 months after the initial antibiotics treatment. d)Post-antibiotics treatment semen analysis was performed on the patient who had no bacterial reinfection at 3 months after the initial antibiotics treatment. e)p-vlaues <0.05 are printed in bold characters.
Table 4
Logistic analysis of bacterial species significantly influencing thespecific semen parameters of subfertile males
- 1. Gnoth C, Godehardt E, Frank-Herrmann P, Friol K, Tigges J, Freundl G. Definition and prevalence of subfertility and infer-tility. Hum Reprod 2005;20:1144-7. ArticlePubMed
- 2. Agarwal A, Mulgund A, Hamada A, Chyatte MR. A unique view on male infertility around the globe. Reprod Biol Endocrinol 2015;13:37. ArticlePubMedPMCPDF
- 3. Han H, Liu S, Zhou XG, Tian L, Zhang XD. Aetiology of obstruc-tive azoospermia in Chinese infertility patients. Andrologia 2016;48:761-4. ArticlePubMed
- 4. Lackner J, Schatzl G, Horvath S, Kratzik C, Marberger M. Value of counting white blood cells (WBC) in semen samples to predict the presence of bacteria. Eur Urol 2006;49:148-52. discussion 152-3. ArticlePubMed
- 5. Punab M, Loivukene K, Kermes K, Mändar R. The limit of leucocytospermia from the microbiological viewpoint. Andro-logia 2003;35:271-8. ArticlePDF
- 6. Pajovic B, Radojevic N, Vukovic M, Stjepcevic A. Semen analysis before and after antibiotic treatment of asymptomatic Chlamydia- and Ureaplasma-related pyospermia. Andrologia 2013;45:266-71. ArticlePubMed
- 7. Zhang F, Dai J, Chen T. Role of Lactobacillus in female infertility via modulating sperm agglutination and immobilization. Front Cell Infect Microbiol 2021;10:620529. ArticlePubMedPMC
- 8. Fraczek M, Kurpisz M. Mechanisms of the harmful effects of bacterial semen infection on ejaculated human spermatozoa: potential inflammatory markers in semen. Folia Histochem Cytobiol 2015;53:201-17. ArticlePubMed
- 9. Allow AK, Abdulmogny ASS, Maryam B, Alaw BA. Sperm agglutination, sperm shaky head movement and sperm-cervi-cal interaction tests could be enough for diagnosis of immunological infertility? J Gynecol Womens Health 2017;3:555603. Article
- 10. Volz Y, Ebner B, Pfitzinger P, Berg E, Lellig E, Marcon J, et al. Asymptomatic bacteriospermia and infertility-what is the connection? Infection 2022;50:1499-505. ArticlePubMedPMCPDF
- 11. Gimenes F, Souza RP, Bento JC, Teixeira JJ, Maria-Engler SS, Bonini MG, et al. Male infertility: a public health issue caused by sexually transmitted pathogens. Nat Rev Urol 2014;11:672-87. ArticlePubMedPDF
- 12. Fraczek M, Hryhorowicz M, Gill K, Zarzycka M, Gaczarzewicz D, Jedrzejczak P, et al. The effect of bacteriospermia and leukocytospermia on conventional and nonconventional semen parameters in healthy young normozoospermic males. J Reprod Immunol 2016;118:18-27. ArticlePubMed
- 13. Wogatzky J, Wirleitner B, Stecher A, Vanderzwalmen P, Neyer A, Spitzer D, et al. The combination matters--distinct impact of lifestyle factors on sperm quality: a study on semen analysis of 1683 patients according to MSOME criteria. Reprod Biol Endocrinol 2012;10:115. ArticlePubMedPMC
- 14. Pluddemann A. Can drinking more water prevent urinary tract infections? The evidence says yes. BMJ Evid Based Med 2019;24:191-2. ArticlePubMed
- 15. Eini F, Kutenaei MA, Zareei F, Dastjerdi ZS, Shirzeyli MH, Salehi E. Effect of bacterial infection on sperm quality and DNA fragmentation in subfertile men with Leukocytospermia. BMC Mol Cell Biol 2021;22:42. ArticlePubMedPMCPDF
- 16. Domes T, Lo KC, Grober ED, Mullen JB, Mazzulli T, Jarvi K. The incidence and effect of bacteriospermia and elevated seminal leukocytes on semen parameters. Fertil Steril 2012;97:1050-5. ArticlePubMed
- 17. Machado A, Cerca N. Influence of biofilm formation by Gard-ne-rella vaginalis and other anaerobes on bacterial vaginosis. J Infect Dis 2015;212:1856-61. ArticlePubMed
- 18. Farahani L, Tharakan T, Yap T, Ramsay JW, Jayasena CN, Minhas S. The semen microbiome and its impact on sperm function and male fertility: a systematic review and meta-analysis. Andrology 2021;9:115-44. ArticlePubMedPDF
- 19. Bai S, Li Y, Hu MH, Wu L, Shui LJ, Wang XH, et al. Association of sexually transmitted infection with semen quality in men from couples with primary and secondary infertility. Asian J Androl 2022;24:317-22. ArticlePubMed
- 20. Toren P, Margel D, Kulkarni G, Finelli A, Zlotta A, Fleshner N. Effect of dutasteride on clinical progression of benign prostatic hyperplasia in asymptomatic men with enlarged prostate: a post hoc analysis of the REDUCE study. BMJ 2013;346:f2109. ArticlePubMedPMC
- 21. Said MA, Mehta A. The impact of 5α-reductase inhibitor use for male pattern hair loss on men's health. Curr Urol Rep 2018;19:65. ArticlePubMedPDF
- 22. La Vignera S, Condorelli RA, Balercia G, Vicari E, Calogero AE. Does alcohol have any effect on male reproductive function? A review of literature. Asian J Androl 2013;15:221-5. ArticlePubMedPMC
REFERENCES
Figure & Data
REFERENCES
Citations
Citations to this article as recorded by 
 ePub Link
ePub Link Cite
CiteImpact of Microbial Infection on Sperm Parameters of Seminal Bacteria in Asymptomatic Subfertile Males
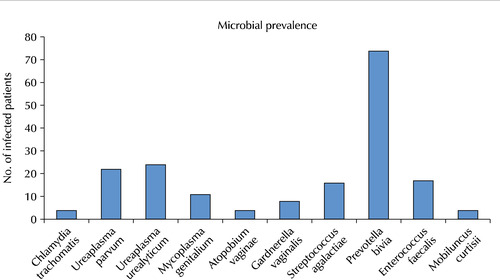
Fig. 1
Prevalence of microbial species in semen samples of subfertile males.
Fig. 1
Impact of Microbial Infection on Sperm Parameters of Seminal Bacteria in Asymptomatic Subfertile Males
Basic characteristics of the subfertile males (n=510)
| Total (n=510) | Bacteriospermic subfertile males (n=179) | Non-bacteriospermic subfertile males (n=331) | p-valuea) | |
|---|---|---|---|---|
| Age (y) | 36.6±6.9 (29-44) | 37.3±6.8 (30-44) | 36.1±7.1 (29-43) | 0.510 |
| Underlying disease history | 0.001 | |||
| Hypertension | 10 (2.0) | 3 (1.7) | 7 (2.1) | 0.021 |
| Chronic prostatitis | 0 (0.0) | 0 (0.0) | 0 (0.0) | - |
| Cerebrovascular disease | 2 (0.4) | 0 (0.0) | 2 (0.6) | 0.056 |
| Diabetes mellitus | 24 (4.7) | 19 (10.6) | 5 (1.5) | <0.001 |
| Presence of LUTS | 0 (0.0) | 0 (0.0) | 0 (0.0) | - |
| Previous history of genital surgery | 0.797 | |||
| Spermatocelectomy | 0 (0.0) | 0 (0.0) | 0 (0.0) | |
| Hydrocelectomy | 9 (1.8) | 3 (1.7) | 6 (1.8) | |
| Orchiopexy | ||||
| Due to testicular torsion | 0 (0.0) | 0 (0.0) | 0 (0.0) | |
| Due to testicular cryptorchidism | 2 (0.4) | 1 (0.6) | 1 (0.3) | |
| Varicocelectomy | 13 (2.5) | 5 (2.8) | 8 (2.4) | |
| Medical treatment prior to the first visit | ||||
| Clomiphene citrate | 0 (0.0) | 0 (0.0) | 0 (0.0) | - |
| Testosterone replacement therapy | 0 (0.0) | 0 (0.0) | 0 (0.0) | - |
| Initial hormone level | ||||
| FSH (mIU/ml) | 5.2±1.5 | 5.1±1.4 | 5.4±0.9 | 0.151 |
| LH (mIU/ml) | 3.8±1.9 | 3.9±1.3 | 3.7±1.7 | 0.337 |
| Testosterone (ng/ml) | 4.8±1.4 | 5.0±1.2 | 4.7±1.1 | 0.242 |
| Prolactin (ng/ml) | 5.6±2.3 | 5.4±2.2 | 5.9±1.9 | 0.508 |
| Semen parameters | ||||
| Volume (ml) | 3.0±2.2 | 2.9±1.7 | 3.6±1.5 | 0.196 |
| Sperm concentration (106/ml) | 46.2±23.6 | 43.3±17.4 | 47.8±20.2 | 0.655 |
| Total motility (%) | 30.0±12.9 | 20.4±10.0 | 36.0±8.6 | <0.001 |
| Progressive motility (%) | 18.1±7.1 | 11.1±5.3 | 22.5±4.7 | <0.001 |
| Leukocytospermia (106/ml) | 0.8±2.1 | 2.8±1.9 | 0.3±0.2 | 0.001 |
| DNA Fragmentation (%) | 32.4±15.2 | 43.2±13.8 | 30.7±11.5 | <0.001 |
| Normal morphology (%) | 2.1±2.3 | 1.5±1.2 | 2.4±1.5 | 0.239 |
| Vitality (%) | 53.0±9.7 | 51.7±6.1 | 55.9±8.4 | 0.575 |
| Microscopic hematuria | <0.001 | |||
| Overall | 125 (24.5) | 115 (64.2) | 10 (3.0) | |
| Grade, RBCs/HPF | ||||
| 0-3 | 100 (19.6) | 93 (51.9) | 7 (2.1) | |
| 4-10 | 20 (3.9) | 17 (9.5) | 3 (0.9) | |
| 11-25 | 5 (1.0) | 5 (2.8) | 0 (0.0) | |
| 26-50 | 0 (0.0) | 0 (0.0) | 0 (0.0) | |
| Semen pathogen PCR analysis | ||||
| Pathogen spectrum | ||||
| Escherichia coli | 0 (0.0) | |||
| Chlamydia trachomatis | 4 (2.2) | |||
| Neisseria gonorrhoeae | 0 (0.0) | |||
| Ureaplasma parvum | 22 (12.3) | |||
| Ureaplasma urealyticum | 24 (13.4) | |||
| Mycoplasma genitalium | 11 (6.1) | |||
| Mycoplasma hominis | 0 (0.0) | |||
| Trichomonas vaginalis | 0 (0.0) | |||
| Gardnerella vaginalis | 8 (4.5) | |||
| Treponema pallidum | 0 (0.0) | |||
| Candida albicans | 0 (0.0) | |||
| Haemophilus ducreyi | 0 (0.0) | |||
| Atopobium vaginae | 4 (2.2) | |||
| Streptococcus agalactiae | 16 (8.9) | |||
| Prevotella bivia | 74 (41.3) | |||
| Pseudomonas aeruginosa | 0 (0.0) | |||
| Klebsiella pneumoniae | 0 (0.0) | |||
| Enterococcus faecalis | 17 (9.5) | |||
| Staphylococcus aureus | 0 (0.0) | |||
| HSV1 | 0 (0.0) | |||
| HSV2 | 0 (0.0) | |||
| Bacteroides fragilis | 0 (0.0) | |||
| Mobiluncus curtisii | 4 (2.2) | |||
| Mobiluncus mulieris | 0 (0.0) | |||
| Multi-microbialb) | 21 (11.7) | |||
| Pathogen presence in semen, overall | 179 (100.0) | - | ||
| Multi-microbial | 21 (11.7) | |||
| Mono-microbial | 158 (88.3) | |||
| Average alcohol consumptionc) | <0.001 | |||
| 0 drinks/wk | 121 (23.7) | 23 (12.8) | 98 (29.6) | |
| 1-15 drinks/wk | 151 (29.6) | 19 (10.6) | 132 (39.9) | |
| >15 drinks/wk | 238 (46.7) | 137 (76.5) | 101 (30.5) | |
| Smoking history | 0.576 | |||
| Never smoked | 350 (68.6) | 125 (69.8) | 225 (68.0) | |
| Current smoker | 97 (19.0) | 34 (19.0) | 63 (19.0) | |
| Previous smoker (current non-smoker) | 63 (12.4) | 20 (11.2) | 43 (13.0) | |
| 5-alpha reductase inhibitor treatmentd) | 109 (21.4) | 29 (16.2) | 80 (24.2) | 0.039 |
Values are presented as mean±standard deviation (range), number (%), or mean±standard deviation.
LUTS: lower urinary tract symptoms, FSH: follicle-stimulating hormone, LH: luteinizing hormone, DNA: deoxyribonucleic acid, RBCs/HPF: red blood cells/high-power field, PCR: polymerase chain reaction, HSV1: Herpes simplex type-1, HSV2: Herpes simplex type-2, –: not available.
a)p-vlaues <0.05 are printed in bold characters. b)Multi-microbial indicates equal or more than 2 bacterial species present in body fluid. c)1 drink is equivalent to 1 glass of wine or 1 single spirit. d)5-alpha reductase inhibitor was used for the treatment of androgenic alopecia.
Antibiotic sensitivity of pathogens detected in urine or semen samples of subfertile males
| C. trachomatis (n=4) | U. parvum (n=22) | U. urealyticum (n=24) | M. genitalium (n=11) | G. vaginalis (n=8) | A. vaginae (n=4) | S. agalactiae (n=16) | P. bivia (n=74) | E. faecalis (n=17) | M. curtisii (n=4) | |
|---|---|---|---|---|---|---|---|---|---|---|
| Ampicillin | N/A | N/A | N/A | N/A | ||||||
| Sensitive | - | - | - | - | 5 (62.5) | 4 (100.0) | 16 (100.0) | 41 (55.4) | 17 (100.0) | 1 (25.0) |
| Intermediate | - | - | - | - | 1 (12.5) | 0 (0.0) | 0 (0.0) | 10 (13.5) | 0 (0.0) | 0 (0.0) |
| Resistant | - | - | - | - | 2 (25.0) | 0 (0.0) | 0 (0.0) | 23 (31.1) | 0 (0.0) | 3 (75.0) |
| Amoxicillin | N/A | N/A | N/A | N/A | N/A | |||||
| Sensitive | 2 (50.0) | - | - | - | 5 (62.5) | 4 (100.0) | 16 (100.0) | 45 (60.8) | - | - |
| Intermediate | 0 (0.0) | - | - | - | 1 (12.5) | 0 (0.0) | 0 (0.0) | 8 (10.8) | - | - |
| Resistant | 2 (50.0) | - | - | - | 2 (25.0) | 0 (0.0) | 0 (0.0) | 21 (28.4) | - | - |
| Ceftriaxone | N/A | N/A | N/A | |||||||
| Sensitive | 3 (75.0) | - | - | - | 7 (87.5) | 4 (100.0) | 16 (100.0) | 59 (79.7) | 0 (0.0) | 3 (75.0) |
| Intermediate | 0 (0.0) | - | - | - | 0 (0.0) | 0 (0.0) | 0 (0.0) | 2 (2.7) | 0 (0.0) | 0 (0.0) |
| Resistant | 1 (25.0) | - | - | - | 1 (12.5) | 0 (0.0) | 0 (0.0) | 13 (17.6) | 17 (100.0) | 1 (25.0) |
| Clarithromycin | N/A | N/A | N/A | |||||||
| Sensitive | 4 (100.0) | 10 (45.5) | 12 (50.0) | 5 (45.5) | 6 (75.0) | 4 (100.0) | - | - | - | 4 (100.0) |
| Intermediate | 0 (0.0) | 1 (4.5) | 0 (0.0) | 1 (9.0) | 0 (0.0) | 0 (0.0) | - | - | - | 0 (0.0) |
| Resistant | 0 (0.0) | 11 (50.0) | 12 (50.0) | 5 (45.5) | 2 (25.0) | 0 (0.0) | - | - | - | 0 (0.0) |
| Clindamycin | ||||||||||
| Sensitive | 2 (50.0) | 9 (40.9) | 11 (45.8) | 5 (45.5) | 7 (87.5) | 4 (100.0) | 14 (87.5) | 74 (100.0) | 3 (17.6) | 4 (100.0) |
| Intermediate | 0 (0.0) | 2 (9.1) | 0 (0.0) | 0 (0.0) | 0 (0.0) | 0 (0.0) | 0 (0.0) | 0 (0.0) | 0 (0.0) | 0 (0.0) |
| Resistant | 2 (50.0) | 11 (50.0) | 14 (58.3) | 6 (54.5) | 1 (12.5) | 0 (0.0) | 2 (12.5) | 0 (0.0) | 14 (82.4) | 0 (0.0) |
| Amikacin | N/A | N/A | N/A | |||||||
| Sensitive | 4 (100.0) | 22 (100.0) | 24 (100.0) | 11 (100.0) | 8 (100.0) | 4 (100.0) | 16 (100.0) | - | - | - |
| Intermediate | 0 (0.0) | 0 (0.0) | 0 (0.0) | 0 (0.0) | 0 (0.0) | 0 (0.0) | 0 (0.0) | - | - | - |
| Resistant | 0 (0.0) | 0 (0.0) | 0 (0.0) | 0 (0.0) | 0 (0.0) | 0 (0.0) | 0 (0.0) | - | - | - |
| Doxycycline | N/A | |||||||||
| Sensitive | 4 (100.0) | 22 (100.0) | 24 (100.0) | 10 (90.9) | 1 (12.5) | 4 (100.0) | 2 (12.5) | - | 5 (29.4) | 2 (50.0) |
| Intermediate | 0 (0.0) | 0 (0.0) | 0 (0.0) | 0 (0.0) | 1 (12.5) | 0 (0.0) | 0 (0.0) | - | 0 (0.0) | 0 (0.0) |
| Resistant | 0 (0.0) | 0 (0.0) | 0 (0.0) | 1 (9.1) | 6 (75.0) | 0 (0.0) | 14 (87.5) | - | 12 (70.6) | 2 (50.0) |
| Ciprofloxacin | N/A | N/A | ||||||||
| Sensitive | 3 (75.0) | 10 (45.5) | 10 (41.7) | 4 (36.4) | 3 (37.5) | 3 (75.0) | 15 (93.8) | - | 0 (0.0) | - |
| Intermediate | 0 (0.0) | 0 (0.0) | 2 (8.3) | 3 (27.3) | 0 (0.0) | 0 (0.0) | 0 (0.0) | - | 0 (0.0) | - |
| Resistant | 1 (25.0) | 12 (54.5) | 12 (50.0) | 4 (36.4) | 5 (62.5) | 1 (25.0) | 1 (6.2) | - | 17 (100.0) | - |
| Metronidazole | N/A | N/A | N/A | N/A | N/A | |||||
| Sensitive | - | - | - | - | 3 (37.5) | 2 (50.0) | 0 (0.0) | 74 (100.0) | - | 0 (0.0) |
| Intermediate | - | - | - | - | 0 (0.0) | 0 (0.0) | 0 (0.0) | 0 (0.0) | - | 0 (0.0) |
| Resistant | - | - | - | - | 5 (62.5) | 2 (50.0) | 16 (100.0) | 0 (0.0) | - | 4 (100.0) |
| Piperacillin/tazobactam | N/A | N/A | N/A | N/A | N/A | |||||
| Sensitive | - | - | - | - | 8 (100.0) | - | 16 (100.0) | 74 (100.0) | 17 (100.0) | 4 (100.0) |
| Intermediate | - | - | - | - | 0 (0.0) | - | 0 (0.0) | 0 (0.0) | 0 (0.0) | 0 (0.0) |
| Resistant | - | - | - | - | 0 (0.0) | - | 0 (0.0) | 0 (0.0) | 0 (0.0) | 0 (0.0) |
| Ertapenem | N/A | N/A | N/A | N/A | N/A | N/A | ||||
| Sensitive | - | - | - | - | - | - | 16 (100.0) | 74 (100.0) | 17 (100.0) | 4 (100.0) |
| Intermediate | - | - | - | - | - | - | 0 (0.0) | 0 (0.0) | 0 (0.0) | 0 (0.0) |
| Resistant | - | - | - | - | - | - | 0 (0.0) | 0 (0.0) | 0 (0.0) | 0 (0.0) |
Values are presented as number (%).
C. trachomatis: Chlamydia trachomatis, U. parvum: Ureaplasma parvum, U. urealyticum: Ureaplasma urealyticum, M. genitalium: Mycoplasma genitalium, G. vaginalis: Gardnerella vaginalis, A. vaginae: Atopobium vaginae, GBS: Streptococcus agalactiae, P. bivia: Prevotella bivia, E. faecalis: Enterococcus faecalis, M. curtisii: Mobiluncus curtisii, N/A: not applicable, –: not available.
Pre- and post-antibiotics treatment semen parameters in subfertile males with bacteriospermiaa)
| U. parvum | U. urealyticum | M. genitalium | |||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|
|
|
|
|
|||||||||
| Pre-Tx (n=22) | Post-Tx (n=17)d) | p-valuee) | Pre-T x (n=24) | Post-Tx (n=21) | p-value | Pre-Tx (n=11) | Post-Tx (n=10) | p-value | |||
| Semen parametersb) | |||||||||||
| Volume (ml) | 2.1±1.5 | 2.8±0.8 | 0.144 | 2.2±1.9 | 2.7±2.0 | 0.157 | 2.3±1.3 | 2.9±1.6 | 0.209 | ||
| Sperm concentration (106/ml) | 45.0±12.9 | 48.2±13.4 | 0.528 | 44.8±15.5 | 45.0±14.2 | 0.782 | 43.2±17.0 | 45.0±9.7 | 0.611 | ||
| Total motility (%) | 17.8±3.1 | 41.4±5.7 | <0.001 | 17.5±6.9 | 47.0±10.1 | <0.001 | 18.0±7.7 | 42.1±5.4 | <0.001 | ||
| Progressive motility (%) | 7.9±4.3 | 31.7±5.9 | <0.001 | 7.3±8.2 | 37.1±9.6 | <0.001 | 9.2±5.6 | 32.9±6.2 | <0.001 | ||
| Leukocytospermia (106/ml) | 3.0±1.4 | 0.4±0.4 | <0.001 | 3.1±1.6 | 0.3±0.1 | <0.001 | 3.0±1.2 | 0.5±0.2 | <0.001 | ||
| DNA fragmentation (%) | 44.6±10.5 | 30.2±11.5 | <0.001 | 45.7±8.6 | 31.4±5.3 | <0.001 | 43.1±11.9 | 30.3±7.8 | <0.001 | ||
| Normal morphology (%) | 1.1±0.5 | 1.1±0.9 | 0.560 | 1.1±1.3 | 1.2±1.1 | 0.617 | 1.5±0.8 | 1.5±1.0 | 0.770 | ||
| Vitality (%) | 47.9±6.5 | 50.4±7.3 | 0.284 | 45.2±8.4 | 47.5±10.3 | 0.589 | 46.5±6.1 | 49.0±11.4 | 0.331 | ||
| Recurrence of bacterial infectionc) | - | 5 (31.8) | - | 3 (12.5) | - | 1 (9.1) | |||||
| G. vaginalis | A. vaginae | S. agalactiae | |||||||||
| Pre-Tx (n=8) | Post-Tx (n=8) | p-value | Pre-Tx (n=4) | Post-Tx (n=3) | p-value | Pre-Tx (n=16) | Post-Tx (n=16) | p-value | |||
| Semen parametersb) | |||||||||||
| Volume (ml) | 3.1±1.2 | 3.7±1.5 | 0.151 | 3.4±2.8 | 3.5±2.0 | 0.682 | 3.2±0.9 | 3.1±1.5 | 0.701 | ||
| Sperm concentration (106/ml) | 42.7±18.4 | 45.7±.10.5 | 0.553 | 49.9±17.2 | 52.9±10.3 | 0.604 | 39.1±10.9 | 42.1±10.6 | 0.728 | ||
| Total motility (%) | 22.1.±7.3 | 24.1±6.2 | 0.722 | 23.6±3.5 | 23.0±5.1 | 0.916 | 20.7±8.2 | 24.0±5.1 | 0.611 | ||
| Progressive motility (%) | 12.2±3.5 | 14.9±6.1 | 0.619 | 14.0±2.8 | 14.1±4.7 | 0.738 | 10.5±5.4 | 14.8±6.0 | 0.392 | ||
| Leukocytospermia (106/ml) | 2.2±1.7 | 0.2±0.1 | 0.001 | 2.5±1.3 | 0.6±0.2 | 0.001 | 3.5±1.5 | 0.3±0.1 | <0.001 | ||
| DNA fragmentation (%) | 41.9±14.2 | 39.5±12.8 | 0.214 | 41.0±14.3 | 41.8±9.9 | 0.312 | 45.0±9.7 | 43.9±8.6 | 0.151 | ||
| Normal morphology (%) | 1.7±0.6 | 2.9±0.7 | 0.011 | 1.6±0.8 | 1.6±1.1 | 0.701 | 1.0±0.7 | 3.2±0.9 | 0.045 | ||
| Vitality (%) | 52.3±5.0 | 53.1±4.4 | 0.834 | 53.0±1.8 | 54.7±3.1 | 0.613 | 44.5±6.4 | 46.0±8.2 | 0.535 | ||
| Recurrence of bacterial infectionc) | - | 0 (0.0) | - | 1 (25.0) | - | 0 (0.0) | |||||
| P. bivia | E. faecalis | M. curtisii | |||||||||
| Pre-Tx (n=74) | Post-Tx (n=74) | p-value | Pre-Tx (n=17) | Post-Tx (n=17) | p-value | Pre-Tx (n=4) | Post-Tx (n=3) | p-value | |||
| Semen parametersb) | |||||||||||
| Volume (ml) | 2.5±1.4 | 3.0±1.2 | 0.173 | 2.1±0.8 | 2.5±1.4 | 0.383 | 3.1±0.7 | 3.5±0.5 | 0.415 | ||
| Sperm concentration (106/ml) | 31.6±19.1 | 47.9±19.1 | 0.039 | 29.8±11.3 | 51.0±13.2 | 0.022 | 44.0±12.5 | 43.1±13.0 | 0.901 | ||
| Total motility (%) | 16.4±11.7 | 49.3±12.6 | <0.001 | 23.7±4.4 | 40.8±13.4 | <0.001 | 22.4±6.1 | 25.1±7.2 | 0.730 | ||
| Progressive motility (%) | 7.8±4.7 | 39.7±11.8 | <0.001 | 13.6±3.9 | 31.3±5.1 | <0.001 | 11.1±2.7 | 16.3±4.0 | 0.526 | ||
| Leukocytospermia (106/ml) | 3.6±1.1 | 0.3±0.2 | <0.001 | 3.3±1.4 | 0.4±0.3 | <0.001 | 2.6±1.5 | 0.3±0.3 | <0.001 | ||
| DNA fragmentation (%) | 45.1±11.1 | 33.6±9.5 | <0.001 | 43.0±12.4 | 41.7±18.0 | 0.001 | 41.6±7.8 | 41.4±10.8 | 0.796 | ||
| Normal morphology (%) | 1.8±0.5 | 2.0±1.3 | 0.127 | 1.5±1.1 | 1.6±0.9 | 0.636 | 1.6±0.4 | 1.6±0.9 | 0.659 | ||
| Vitality (%) | 48.7±7.2 | 58.0±4.1 | 0.029 | 49.9±5.3 | 59.2±8.4 | 0.018 | 44.9±5.7 | 47.4±9.2 | 0.627 | ||
| Recurrence of bacterial infectionc) | - | 0 (0.0) | - | 0 (0.0) | - | 1 (25.0) | |||||
| Semen parameters | |||||||||||
| Volume (ml) | 2.1±0.9 | 3.0±1.7 | 0.140 | 2.9±1.7 | 3.1±1.4 | 0.507 | |||||
| Sperm concentration (106/ml) | 30.9±16.6 | 32.1±12.6 | 0.609 | 43.3±17.4 | 54.1±15.3 | 0.047 | |||||
| Total motility (%) | 22.1±8.6 | 41.0±10.8 | <0.001 | 20.4±10.0 | 35.8±8.2 | 0.031 | |||||
| Progressive motility (%) | 13.3±4.8 | 32.3±6.1 | <0.001 | 11.1±5.3 | 26.5±6.5 | 0.027 | |||||
| Leukocytospermia (106/ml) | 4.0±0.9 | 0.5±0.2 | <0.001 | 2.8±1.9 | 0.4±0.2 | 0.014 | |||||
| DNA fragmentation (%) | 46.4±8.1 | 42.1±10.1 | 0.129 | 43.2±13.8 | 37.6±10.4 | 0.001 | |||||
| Normal morphology (%) | 1.0±0.7 | 1.2±0.5 | 0.517 | 1.5±1.2 | 1.8±1.0 | 0.464 | |||||
| Vitality (%) | 44.4±5.9 | 46.3±11.7 | 0.805 | 51.7±6.1 | 51.1±7.8 | 0.655 | |||||
| Recurrence of bacterial infectionc) | - | 0 (0.0) | 11 (6.1) | ||||||||
Values are presented as mean±standard deviation or number (%).
U. parvum: Ureaplasma parvum, U. urealyticum: Ureaplasma urealyticum, M. genitalium: Mycoplasma genitalium, G. vaginalis: Gardnerella vaginalis, Tx: treatment, DNA: deoxyribonucleic acid, A. vaginae: Atopobium vaginae, GBS: Streptococcus agalactiae, P. bivia: Prevotella bivia, E. faecalis: Enterococcus faecalis, M. curtisii: Mobiluncus curtisii, C. trachomatis: Chlamydia trachomatis, –: not available.
a)Genitourianry tract bacterial presence indicates bacterial infection confirmed in urine or semen samples. b)Semen parameters are presented in mean±standard deviations. c)Recurrence rate was evaluated at 3 months after the initial antibiotics treatment. d)Post-antibiotics treatment semen analysis was performed on the patient who had no bacterial reinfection at 3 months after the initial antibiotics treatment. e)p-vlaues <0.05 are printed in bold characters.
Logistic analysis of bacterial species significantly influencing thespecific semen parameters of subfertile males
| Semen parameter | Bacterial species | OR | 95% CI | p-valuea) | Bacterial species | OR | 95% CI | p-valuea) | |
|---|---|---|---|---|---|---|---|---|---|
| Semen volume | None | - | - | - | None | - | - | - | |
| Sperm concentration | PB | 0.177 | 0.080-0.903 | 0.002 | PB | 0.122 | 0.019-0.757 | 0.030 | |
| EF | 0.110 | 0.045-0.691 | 0.011 | EF | 0.254 | 0.022-0.823 | 0.039 | ||
| Motility | UP | 0.119 | 0.009-0.618 | 0.021 | UP | 0.349 | 0.016-0.846 | 0.032 | |
| UU | 0.185 | 0.014-0.722 | 0.017 | UU | 0.245 | 0.119-0.531 | 0.040 | ||
| MG | 0.103 | 0.034-0.545 | 0.033 | MG | 0.170 | 0.084-0.789 | 0.041 | ||
| PB | 0.017 | 0.005-0.427 | 0.019 | PB | 0.085 | 0.011-0.332 | 0.027 | ||
| EF | 0.072 | 0.005-0.167 | 0.035 | EF | 0.590 | 0.107-1.092 | 0.077 | ||
| DNA fragmentation | UP | 0.090 | 0.023-0.125 | 0.024 | UP | 0.151 | 0.083-0.199 | 0.036 | |
| UU | 0.078 | 0.012-0.153 | 0.012 | UU | 0.178 | 0.028-0.307 | 0.025 | ||
| MG | 0.193 | 0.091-0.710 | 0.042 | MG | 0.406 | 0.091-1.185 | 0.106 | ||
| PB | 0.088 | 0.060-0.109 | 0.005 | PB | 0.091 | 0.044-0.128 | 0.017 | ||
| Normal morphology | GBS | 0.091 | 0.080-0.096 | 0.036 | GBS | 0.011 | 0.031-1.202 | 0.105 | |
| Vitality | PB | 0.122 | 0.056-0.451 | 0.013 | PB | 0.134 | 0.038-0.703 | 0.029 | |
| EF | 0.011 | 0.003-0.738 | 0.047 | EF | 0.023 | 0.010-0.512 | 0.047 |
OR: odds ratio, 95% CI: 95% confidence interval, PB: Prevotella bivia, EF: Enterococcus faecalis, UP: Ureaplasma parvum, UU: Ureaplasma urealyticum, MG: Mycoplasma genitalium, GBS: Streptococcus agalactiae.
a)p-vlaues <0.05 are printed in bold characters.
Table 1
Basic characteristics of the subfertile males (n=510)
Values are presented as mean±standard deviation (range), number (%), or mean±standard deviation. LUTS: lower urinary tract symptoms, FSH: follicle-stimulating hormone, LH: luteinizing hormone, DNA: deoxyribonucleic acid, RBCs/HPF: red blood cells/high-power field, PCR: polymerase chain reaction, HSV1: Herpes simplex type-1, HSV2: Herpes simplex type-2, –: not available. a)p-vlaues <0.05 are printed in bold characters. b)Multi-microbial indicates equal or more than 2 bacterial species present in body fluid. c)1 drink is equivalent to 1 glass of wine or 1 single spirit. d)5-alpha reductase inhibitor was used for the treatment of androgenic alopecia.
Table 2
Antibiotic sensitivity of pathogens detected in urine or semen samples of subfertile males
Values are presented as number (%). C. trachomatis: Chlamydia trachomatis, U. parvum: Ureaplasma parvum, U. urealyticum: Ureaplasma urealyticum, M. genitalium: Mycoplasma genitalium, G. vaginalis: Gardnerella vaginalis, A. vaginae: Atopobium vaginae, GBS: Streptococcus agalactiae, P. bivia: Prevotella bivia, E. faecalis: Enterococcus faecalis, M. curtisii: Mobiluncus curtisii, N/A: not applicable, –: not available.
Table 3
Pre- and post-antibiotics treatment semen parameters in subfertile males with bacteriospermiaa)
Values are presented as mean±standard deviation or number (%). U. parvum: Ureaplasma parvum, U. urealyticum: Ureaplasma urealyticum, M. genitalium: Mycoplasma genitalium, G. vaginalis: Gardnerella vaginalis, Tx: treatment, DNA: deoxyribonucleic acid, A. vaginae: Atopobium vaginae, GBS: Streptococcus agalactiae, P. bivia: Prevotella bivia, E. faecalis: Enterococcus faecalis, M. curtisii: Mobiluncus curtisii, C. trachomatis: Chlamydia trachomatis, –: not available. a)Genitourianry tract bacterial presence indicates bacterial infection confirmed in urine or semen samples. b)Semen parameters are presented in mean±standard deviations. c)Recurrence rate was evaluated at 3 months after the initial antibiotics treatment. d)Post-antibiotics treatment semen analysis was performed on the patient who had no bacterial reinfection at 3 months after the initial antibiotics treatment. e)p-vlaues <0.05 are printed in bold characters.
Table 4
Logistic analysis of bacterial species significantly influencing thespecific semen parameters of subfertile males
OR: odds ratio, 95% CI: 95% confidence interval, PB: Prevotella bivia, EF: Enterococcus faecalis, UP: Ureaplasma parvum, UU: Ureaplasma urealyticum, MG: Mycoplasma genitalium, GBS: Streptococcus agalactiae. a)p-vlaues <0.05 are printed in bold characters.

